(002).png)
Perspectives of Non-Speaking ICU Patients and their Families on Goals-of-Care and End-of-Life Discussions
Fiona Campbell, PhD,SLP, Reg. CASLPO, Taylor Chan, BSc(Hons), Cheryl Missiuna, PhD, Joseph B. Orange, PhD, Ashwini Namasivayam-Macdonald, PhD, CCC-SLP, SLP(C), Reg. CASLPO and Lyn S. Turkstra, PhD, CCC-SLP, BC-NCD(A)
Abstract
Objectives: The objective of this study was to explore how patients and their caregivers perceived their communication during goals-of-care/end-of-life discussions and decision-making in the intensive care unit (ICU). The patient participants were temporarily non-speaking due to their medical treatment and used augmentative and alternative communication (AAC) during their stay in the ICU. Results from patient participants were garnered when they reported their experience retrospectively. The long-term goal was to support strategies and assist in the development of AAC tools for patient participation during goals-of-care and end-of-life conversations.
Methods: Participants were recruited via study flyer during their ICU stay and included four adults who were admitted to the ICU and intubated, and their family members. Patient and family participants were interviewed separately about their experiences during goals-of-care and end-of-life discussions when patient participants were intubated and unable to participate fully. Interviews occurring when participants were speaking again and no longer in ICU, were audio-recorded, transcribed and analyzed using inductive thematic analysis.
Findings: Participants’ reports of their goals-of-care/end-of-life discussions and decision-making were summarised into five major themes: (a) communication partners, (b) feelings and thoughts, (c) matters to talk about, (d) control/power, and (e) how communication occurs. Theme a (communication partners) depicts patients’ unmet needs and wants and information/explanations from their healthcare providers. Theme b (matters to talk about) summarizes participants’ experiences with ICU care, operations and interventions. Theme c (feelings and thoughts) characterizes participants’ fear, frustration, isolation, wanting to be treated as themselves and ways in which family participants feel overwhelmed. Theme d (control/power) characterizes patient participants’ self determination: they know what they want, are tracking activities in ICU and also question who has control of goals-of-care decision making. Theme e (how communication occurs) includes the sub-themes: safety, no communication and lack of staff understanding. Additional subthemes are unaided and aided communication experiences during goals-of-care/end-of-life discussions.
Conclusions and Implications for Clinical Practice: Results suggest a need exists for tools that include ICU-specific vocabulary and communication partner training, so that non-speaking AAC users can fully participate in their own goals-of-care and end-of-life discussions in the ICU.
Keywords: vocabulary, communication, intensive-care units, delivery of health care, patient care planning.
Implications for Nurses
This study offers insights for critical nurses about the communication needs of non-speaking patients in the ICU. Themes from this study show non-speaking patients in the ICU are tracking their care by monitoring their equipment, medications, and treatments. Patients wish for more information and involvement in their care and treatment discussions and also recognise when medical decisions are made by their family without their involvement.
Results from this study demonstrate AAC systems are not enough: patients need access to more specific ICU vocabulary and caregiver support if they are to participate in goals-of-care and end-of-life discussions.
Understanding patients’ communication needs will help researchers develop a new vocabulary system designed for goals-of-care and end-of-life communication. With such a system, critical care nurses could offer a tool to non-speaking patients, to best support their desire to fully participate in goals-of-care and end-of-life discussions and decision-making while also supporting families during this difficult time.
Background
According to Statistics Canada (2022), 56% of total deaths in Canada occurred in hospital, and in 9% of ICU stays in Canada, the patient died (Canadian Institute Health Information, 2016). In any given hour in a United States ICU, 50% of patients will be intubated (Wunsch et al., 2013), and thus unable to produce voice and rendered effectively non-speaking (Karlsen et al., 2019; Rose et al., 2021). Some ICU patients are unable to meet their needs using natural speech because of an acquired medical condition that gives them a speech and/or language impairment (Zaga et al., 2023). AAC systems help patients communicate. Without access to communication supports, all patients, regardless of the reason they are non-speaking, may be unable to communicate their basic needs (Balandin et al., 2007; Happ et al., 2014; Cheng et al., 2024). If patients do not have access to AAC systems, they rely on substitute decision-makers or use unaided communication, which are both methods that do not fully enable patients to communicate what they want to say (Chidwick et al., 2013; Rodriguez et al., 2015). In addition, non-speaking patients may experience additional feelings of fear, anger and being trapped compared to speaking patients (Khalaila et al., 2011;Tembo et al., 2015). Bartlett et al. (2008) report non-speaking patients have more than twice as many reported adverse medical events because of clinical errors than their speaking counterparts .
According to Ontario’s Health Care Consent Act (1996) all capable patients should give consent for treatments, therapies, and goals of care. Goals-of-care discussions may be considered end-of-life discussions if they involve the plan for a person about whom people would not be “surprised if they died in the next year” (You et al., 2014a, p.426), a common scenario in the ICU as patients are admitted with complex medical conditions. Ideally, goals-of-care and end-of-life wishes are discussed in advance of an ICU admission using advance care directives, but many patients are not prepared or have an unplanned acute medical condition as “no one can foresee, or control events associated with end-of-life care and dying” (Andreassen et al., 2017, p. 3). Therefore, patients may want to express their needs and make decisions about their own care in the midst of their ICU admission.
ICU patients are often supported by family members in their decisions and can be considered relatively autonomous because of their family involvement and influence (Grignoli et al., 2018). Some ICUs rely on substitute decision makers, but there is evidence that providers and family make decisions in line with their own values (Chidwick et al., 2013), which might not reflect those of the patient.
Non-speaking ICU patients can benefit from AAC systems (ten Hoorn et al., 2016; Carruthers et al., 2017; LaValley et al., 2024). AAC comprises the methods, vocabulary, and tools used to help people communicate when they are cognitively capable but non-speaking (Light et al., 2019). AAC uses interfaces which enable patients to select vocabulary they see or hear. An example is the purposefully designed picture-based vocabulary, the Communication Aid to Capacity Evaluation (CACE) (Carling-Rowland et al., 2014). People experiencing aphasia used CACE to demonstrate their capacity when making discharge decisions, but it does not cover other decisions (Carling-Rowland et al., 2014). Researchers have investigated the vocabulary content of AAC speaking applications for ICU patients (Etchels et al., 2013; Kozalinski et al., 2015; Mobasheri et al., 2016), and have found that these have focused on everyday care needs. There have been no studies of the specific vocabulary needed to support goals-of-care/end-of-life discussions and decision-making. It is important to learn from patients and their families about their experiences. There is limited research reported on how non-speaking patients communicate their goals-of-care and end-of-life preferences and decisions using AAC (Torlotti et al., 2023).
Berlin (2017) defined the most important aspects of goals of care discussions “as formulating a shared understanding of the patient’s prognosis, establishing therapeutic rapport, providing emotional support, and probing for patient preferences” (p.1281). Bomhof-Roordink et al. (2019) recommended a shared decision-making model for goals-of-care and end-of-life conversations, as this ensures that the conversation is two-way and reflects the patient’s values, preferences, and questions before decisions are made. If patients who cannot speak simply gesture or answer yes/no questions, they will only be partially able to participate in a shared decision-making process (Rodriguez et al., 2015). Research has shown that partial participation of patients can occur in a couple of ways. First, hospital staff might rely on typing and handwriting, but both may be too difficult and tiring for non-speaking ICU patients (Laerkner et al., 2015). Second, patients may end up with only being informed of goals-of-care decisions after their family and providers have already made the decision for them (Happ et al., 2007). Research on goals-of-care and end-of-life discussions can have a significant impact on healthcare, given the number of people potentially involved in these discussions and those people living with an altered quality of life when discharged following an ICU admission (Nabozny et al., 2016).
Study Objectives
This study aimed to fill the gaps about communication needs in goals-of-care and end-of-life discussions, by interviewing patients and their families about their experiences. Patients and/or families all had some discussions about goals of care when the patient was in the ICU. The interviews in this study took place up to a year after patient discharge from the ICU. The research question was: what are the communication needs of adult patients who are non-speaking, use augmentative and alternative communication, and wish to have quality goals-of-care/end-of-life care conversations? The aim was to identify unmet communication needs that could be supported in the future with goals-of-care/end-of-life AAC vocabulary. This study was designed to be a step toward a long-term goal of supporting full participation of AAC users in goals-of-care/end-of-life discussions.
Method
Study Design
Participants
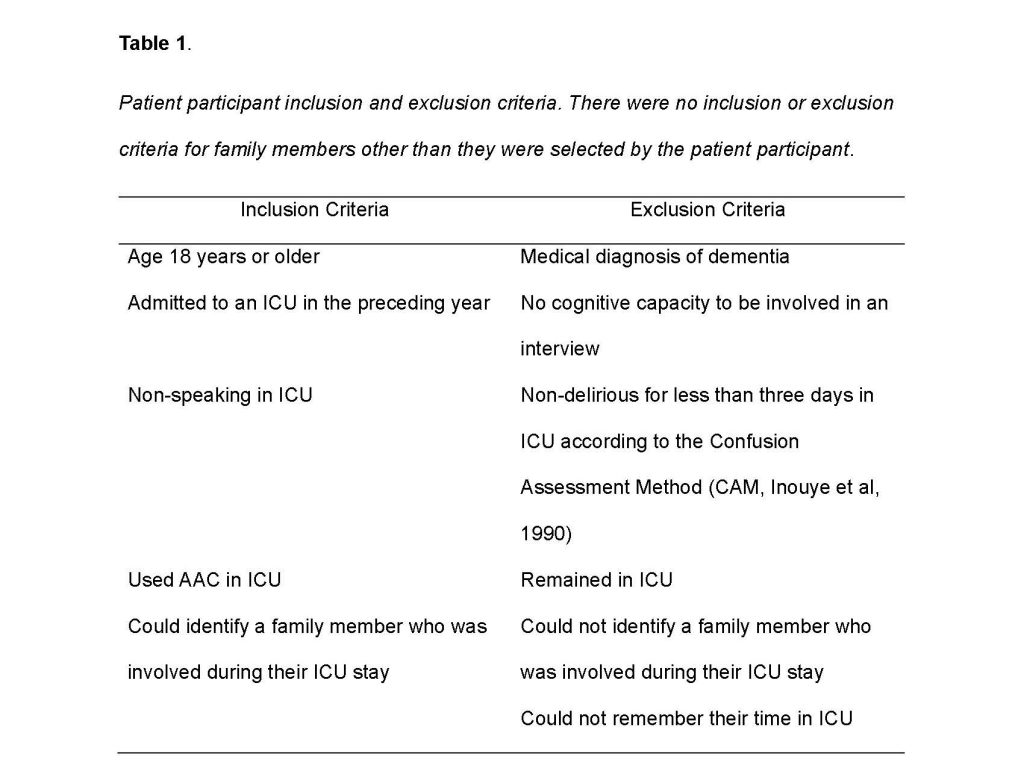
Patient participants were adults who had been ICU patients at a teaching hospital in Ontario, Canada. Healthcare staff invited patients via a study flyer and informed consent process was completed while the patient participants were in ICU by a research staff member who was unknown to the participants. Recruitment and consent processes were approved by the Hamilton Integrated Research Ethics Board (HiREB). Participants were interviewed after discharge from ICU. Patient participant inclusion and exclusion criteria are listed in Table 1. One family participant was nominated by each patient participant who followed the same consent process as the patient participant.
Design
This study used a qualitative, case-study design with semi-structured interviews, to understand the “uniqueness and complexity of the cases, its embeddedness and interaction with its contexts” (Stake,1995; p.16). The interviewer (FC) used her knowledge of augmentative and alternative communication and intensive care units to add follow-up questions and elicit participants’ descriptions of their experiences. FC and co-author TC used thematic content analysis (Braun & Clarke 2006) as its interpretive process is ideal in studies of a phenomenon about which not much is known. Analysis was inductive, i.e., researchers coded what the data showed and then further made sense of the data by cross-referencing to patient participants’ diagnosis, length of time in the intensive care unit, and augmentative and alternative communication system. All methods were approved by the Hamilton Integrated Research Ethics Board (HiREB).
Researchers
FC is a Speech-Language Pathologist (SLP) with a PhD and co-delivers the augmentative and alternative communication service in the intensive care units where the study was conducted. TC was an undergraduate student with volunteer experience at a nursing home but no formal healthcare training. LT is an SLP researcher specializing in long-term outcomes after acquired brain injury with minimal augmentative and alternative communication in the intensive care unit experience.
Interview Methods
Semi-structured interview questions were used to probe each patient’s experience while non-speaking and using AAC when (a) directing their care, (b) engaging in a discussion of their goals of care with family or staff on a one-to-one basis, (c) having a family meeting to discuss care, and (d) completing the Physician Order Scope of Treatment (POST) with healthcare staff. Patient and family-member participants were asked to describe their experiences when the intubated patient was not able to talk in the ICU and to discuss whether the patient was able to tell people what they needed. Participants were asked retrospectively to name the patient’s treatments, including any operations; what treatments they discussed; and with whom they discussed those treatments. Participants were asked about positive and negative aspects of those discussions; participants’ level of inclusion; ideas left unsaid; and any aspects of the treatment discussion participants wished they could have changed. Finally, participants were asked about transitioning from discussions to making decisions about goals of care/end of life, and if those decisions reflected the patient’s wishes and opinions. Interview questions are listed in Appendix A.
Data Processing
Interviews were audio recorded using an Audacity sound recorder on a Dell ProBook computer. Recordings were uploaded to Microsoft Office 365 for auto-transcription (without storage) using the Microsoft server (https://eastus.api.cognitive.microsoft.com), All identifying information was removed, IDs were coded, and audio files were destroyed. Coded, de-identified transcripts were uploaded to Dedoose (2015) software for analysis.
Data Analysis
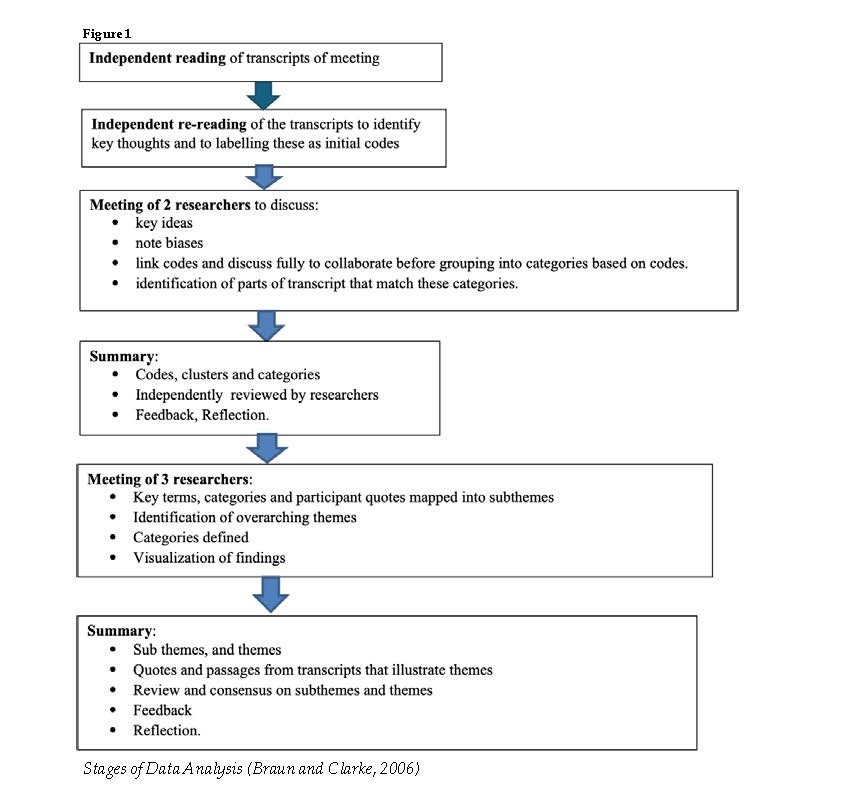
Thematic analysis followed the stages shown in Figure 1 (Braun & Clarke 2006).
Researchers FC and TC independently read all transcripts, identified key concepts in the data, and labelled those as initial codes for two transcripts each. Codes were compared (i.e., match vs. mismatch) and grouped to create the final code tree of categories and subcategories (see Supplementary Materials Table 1). A consensus process was used to obtain final agreement (Richard & Hemphill, 2017): (a) the two researchers both coded the transcripts for participants 001, 002, 003, and 004, (b) they met to discuss the data and where the code was applied, (c) they coded the same transcripts for family members (002-2, 003-2), (d) they met again to discuss the data and use of the code tree, and (e) they finished coding transcripts from the remaining participants. Coding of participant 001-2 was completed by FC.
After coding was complete, the two researchers met with a third researcher (LT) to re-examine the data and identified any coded sub-categories with more than 30 quotes as important. Excerpts that “stood out” from the evidence, including views strongly expressed, repeated statements that represented common ideas across a group of people, and statements that highlighted an unmet communication need were noted. Researchers were emailed illustrative excerpts in a table, along with another table of subcategories not reviewed in the meeting and all three researchers gave written feedback.
Data Verification and Consistency of Analysis
Transcription fidelity was verified by TC and FC via comparison of transcripts to audio recordings. Transparency and consistency of the analysis was ensured by having two researchers first blindly coding the same research data, then meeting to establish a clear protocol and codebook (Gibbert et al., 2008) and adding a consensus process in application of the code tree.
Findings
Four patient participants met inclusion criteria (see Table 2) and each of them nominated one family member who they recall supported them in the intensive care unit at the time of their admission. No participants dropped out. The eight patient and family participants were interviewed by author FC in a private, quiet location in a hospital, rehabilitation, or community setting, less than one year after their intensive care unit discharge date. All patient participants had been loaned an aided communication system during their intensive care unit stay. These aided systems were either high technology (via speaking software on a computer) or low technology (via a communication book and alphabet chart). One participant had a camera mounted on the computer to track their head movements and control the mouse cursor. By hovering the mouse cursor over the letter or phrase the participant was able to make a selection that was spoken out loud by the speaking software. Another participant waited for the computer to highlight different vocabulary options and then pressed a switch to select their choice. Participants using the communication book listened to the vocabulary spoken out loud one phrase at a time and then gestured “yes” to make a choice. They also could listen to letter choices and gesture “yes’ to select one letter at a time.
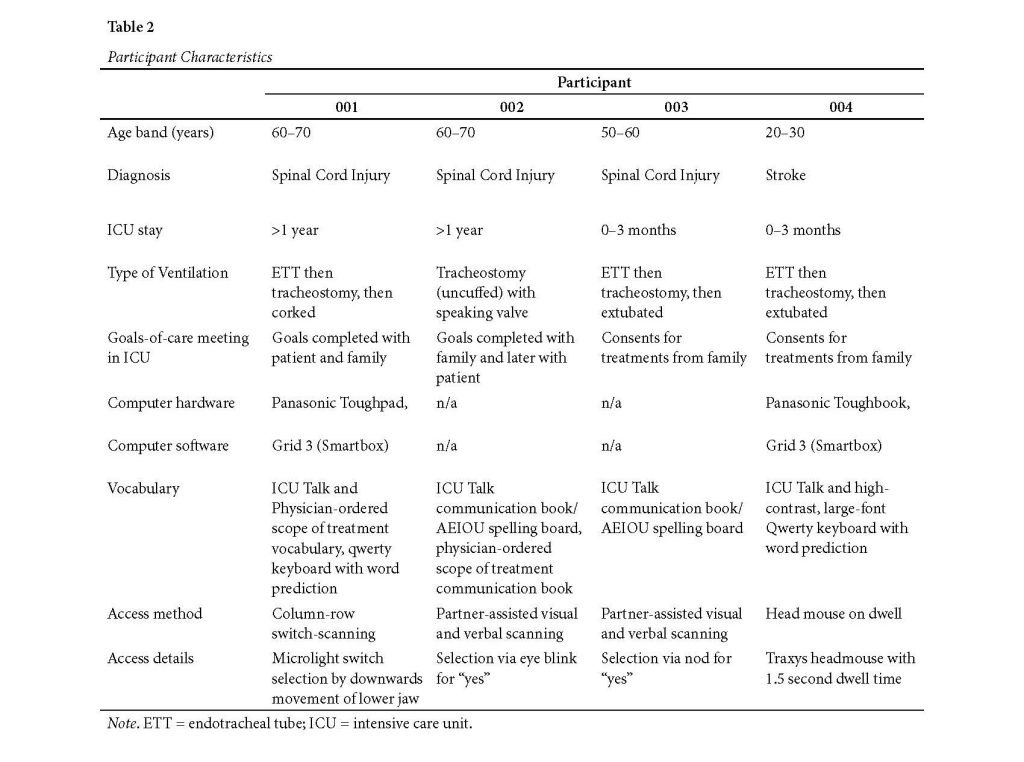
Each aided system was prescribed by an SLP and OT and implemented by health care staff on the unit after receiving training. The equipment was assigned to the patient and available for use at all times. During their ICU stay, all participants were both mechanically ventilated and tetraplegic. Before and after their intensive care unit stay, all participants were talking. During the interviews, all participants were talking.
Participants’ reports of their goals-of-care/end-of-life discussions and decision- making were summarised into five major themes: (a) communication partners, (b) feelings and thoughts, (c) matters to talk about, (d) control/power, and (e) how communication occurs. These themes were cross-referenced to electronic medical record data on patients’ mechanical ventilation, augmentative and alternative communication system, and goals-of-care/end-of-life meetings. Themes and subthemes are summarized in Table 3, and details and quotes are provided below.
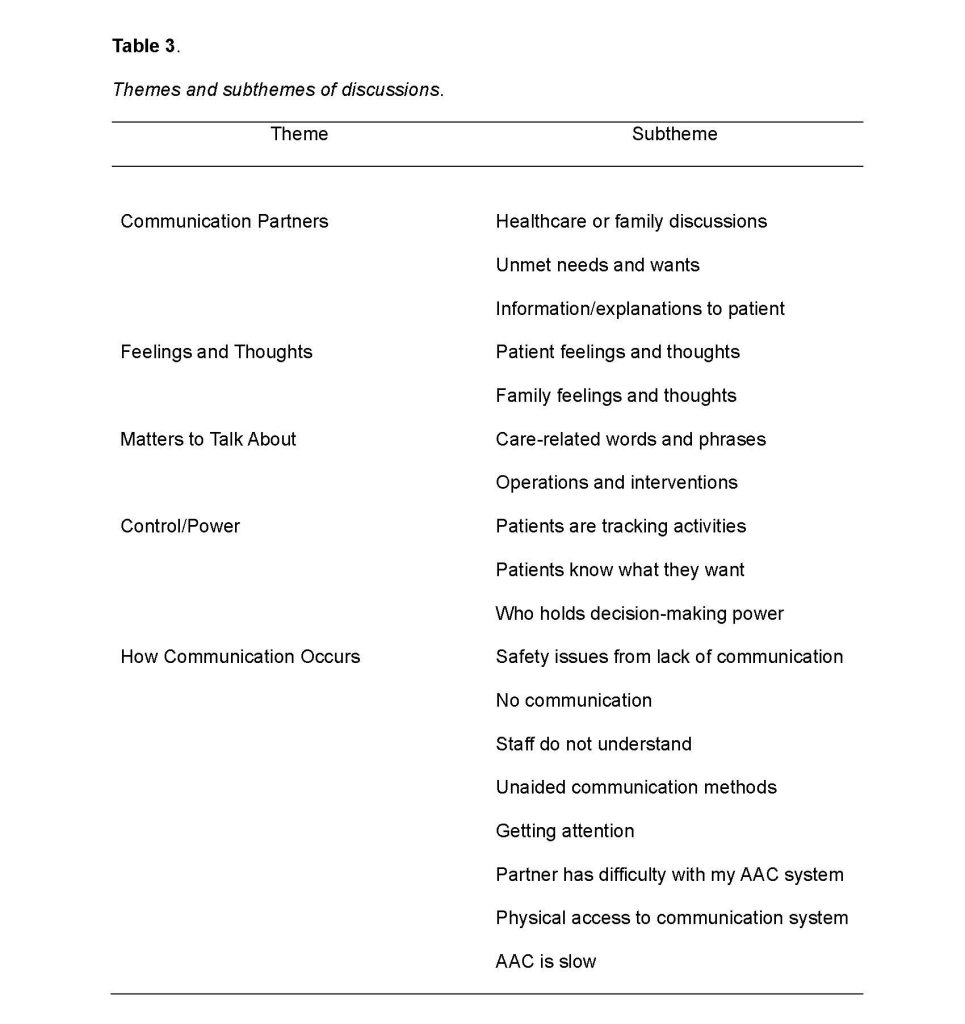
Theme A: Communication Partners
Subthemes: Healthcare Worker and Family Discussions, Unmet Needs and Wants and Information/Explanations to Patients.
Patients’ communication partners were health care staff, family and sometimes friends who visited them in the intensive care unit. Two participants reported goals-of-care/end-of-life meetings: one with both the family and patient participant; and one with the family participant first and the patient participant afterwards. For the remaining participants, goals-of-care/end-of-life discussion was limited to consent for specific surgeries and interventions. One family participant said they were informed about lifesaving measures after the fact without having decided on care specifics, such as ventilation, when they initially agreed to the surgery. Two family participants reported social workers and nursing staff enhanced their understanding of medical information and reduced their distress. Two patient participants appreciated nurses keeping their family members “in the loop” on medical decisions and one family participant felt staff could learn by listening. Onefamily participant received information shortly after the patient was admitted to the Intensive Care Unit, but was not ready to take it in:
I guess some of the communications I don’t, for me, I don’t believe sank in. I mean at that point my thought was to sustain life. No idea where that could lead us down the road to a ventilator (P002-2).
Two family participants said they ignored negative messages and preferred to hear positive, reassuring messages. Twofamily participant’s rehabilitation pathway described by their surgeon did not match reality, with delays in transfers and discharges. All four patient participants described multiple surgeries and interventions, with varied outcomes that were unexpected such as new medications and further operations that were not initially described by healthcare staff. One patient participant reported they were under-prepared for the pain of certain procedures.One family participant was familiar with healthcare but for others everything was new and required them to learn a lot of new information. An example was learning about mechanical ventilation:
“They [my family] did not have any idea what [mechanical ventilation] was all about until they were told I was going to be on it for life and that a lot of the care in hospital was about the breathing tube” (P001).
Patients reported difficulty meeting their basic needs. Onepatient participant’s basic care happened automatically. Other patient participants found care was not always delivered when they needed it. Patients sometimes had unforeseen needs, and until they had an augmentative and alternative communication system, they could not tell people what they needed: “I’m extremely uncomfortable, my neck hurts in this position, but I can’t express that unless someone gets here and I’m like please turn me, like with my eyes” (P004). One family participant recommended that staff do hourly check-ins, asking the patient detailed questions, especially regarding position changes and pressure sores (reported by another family participant).Nurses were the consistent source of information for two patient and family participants, who were not local and could miss the physician’s visits. One family member would read the patient’s lips, acting as a translator during goals-of-care/end-of-life discussions. Sometimes a key person for the patient, such as a nurse, would act as a liaison between the patient and their doctors: “I really appreciate her for that. If the charge nurse didn’t know she would go and find out” (P001). Two patient participants said they loved their doctor, would have liked to have seen them more, and appreciated their doctor’s honesty and direct communication. One family participant blocked patient direct-contact with medical residents to avoid patient distress. One participant reported difficulties relaying their symptoms, asking questions, and communicating what care they wanted to their physicians.Family and patient participants made suggestions to improve their doctor’s style of communication:
To be positive…You’re never going to walk again as negative. We don’t believe you’re going to walk again; all indications show you’re not going to walk again so couch it a little bit more (P002-2).
Healthcare staff may know a diagnosis but need to be careful.
The ICU stay is a time of much new learning and information for the patient, and repetition can be helpful. As one patient participant said, “He [the OT] came back a couple of times to help [with computer speaking software] because it took a couple of visits to get the hang of that” (P001).
Theme B: Feelings and Thoughts
Patient participants said they were unable to do things for themselves as easily as before because they could not move or speak, so they could be fearful of time left alone or having equipment used on them that might fail, such as the Hoyer lift that is used for transfers from bed to another location (e.g., a wheelchair). After hearing about having quadriplegia, one family participant reported that the patient said, “I’m a burden, I’m just a talking head, all I do is eat and poop” (P003-2). Patient participants appreciated people talking to them and wanted to be treated as themselves: “I wanted them to treat me like I was me because I still was” (P001).Patient participants described feeling frustrated. As P004 said, “I felt very trapped in my body”. Patient participants’ communication difficulties caused isolation, and they found it hard to be reliant on their communication partners to help them communicate: “I have all the time in the world like we’re going to go through this alphabet slowly instead of waiting for the right question” (P004). Patient participant (P001) reported that interventions were done to them, without them knowing – “So, I felt like that was taking away my control and I care all about that” – but they wanted to make choices about their care and discharge locations. One patient participant did not want their family to leave and appreciated family support.
The two family members of patients who had been in the ICU longer than a year were assigned a key worker who was a charge nurse or social worker and ensured patient-led questions were answered, families received updated information, and discharge planning was facilitated. A patient who was in the ICU for a shorter time, had an “involved” Intensivist who provided this information.
Two family participants mentioned the importance of ICU and surgical staff considering not only the information they were conveying but also how their comments would make patients and families feel:
Doctor told us maybe that was his job, I didn’t appreciate it, and I have no time for him because he’s too negative…take a sales course to sell it a little better, that’s been devastating the first night to hear that (P002-2).
One family participant said looking up and understanding the medical facts was not enough. Empathy and listening were important too: “they should put themselves in our shoes and [consider] family member knows too” (P004-2). All family participants said that staff should be careful when they were explaining matters to patients. Patients could get upset when they indirectly overheard medical discussions. Change is not just experienced by the patient: family members also had to deal with significant changes in the patient and could feel overwhelmed: “I was upset when they wanted to put the trache[ostomy] in because I thought oh my God, they’re going to think this is permanent like you know so many quads have a trache and it’s just overwhelming” (P003-2). Family members did not always take in the information given to them or believe what they were told by physicians.
Theme C: Matters to Talk About
All participants talked about ICU-specific topics, words, and phrases needed for communication about daily care, surgical operations, and invasive and non-invasive interventions. Two patient participants experienced pain that was not always managed: “I kind of went through withdrawal, but I really needed a nurse, but I couldn’t say anything” (P004). Pain medications sometimes varied by too much or too little, but they were unable to direct their medication: “The doctor on the floor refused medication for me to sleep” (P002). Allpatient participants said they were aware of their suction rehabilitation goals e.g., “I had to get working on 2 or 3 points to get my suctioning down to twice a day “(P001). All patient participants felt urgency when it was hard to breathe: “Like I remember lying down and it being really hard to breathe, and I was like ‘oh I need suction’, like I need suction immediately” (P004).Patient participants described having surgeries, such as spinal surgery, tracheostomies, insertion of PEG tubes and drains, and diagnostic tests. One family participant remembered how life-saving decisions were made and reflected on how major those decisions were: “I think the surgeon initially made the big decision that he needed to go in and secure the neck, that surgery would have been a major decision to move forward” (P002-2). Patient participants did not like the endotracheal tube (ETT) for ventilation: “I was like please get this out of me I want the trache[ostomy] and PEG” (P004). When they were weaned off the tracheostomy, one participant said they wanted the process to go faster. Two patients found weaning too hard and wanted to stop altogether.
One patient and family participant noted the important role of respiratory therapy for weaning the patient off the ventilator and working towards going home. Patient participants were not always pleased with therapy access, plans, or outcomes. Two patient participants did not have access to all the AAC equipment, and reported that they did not have enough physiotherapy and SLP.
Theme D: Control/Power
Subthemes: Patients Know What They Want, Who Holds Decision Making Power and Patients are Tracking Activities
Three patient participants were not given enough information and did not feel they were always in control of the direction of their care: “I was frustrated when I didn’t know. I was like come on tell me” (P004). Patientparticipants wanted to be part of the conversation about their goals of care:, “I like it when they would be like OK, so this is what’s going to happen like this. This is the game plan. I like to be updated because I can’t ask” (P004). All patient participants reported noticing when they did not get to have a say in their care.
I bucked them a lot and I overrode some of the directives they were giving like how long I was supposed to be on cork, how long was I supposed to be on that air machine. I wondered if it was going to get her [the respiratory therapist] in trouble with the physician the next day (P003).
Patient participants showed they knew what they wanted by asking questions using the onscreen keyboard in their AAC system: “Why, I said, are you trying to be weaning me off something you know I have to be on for the rest of my life” (P001). Participants also worried about the reactions of healthcare staff. Sometimes the patient chose to allow their family or a physician to decide for them: “I felt very comfortable with my parents making the decision” (P004). While they allowed other people to decide for them, patients said they still wanted to be informed.
Two patient participants used to be the decider and had lost control over decisions about their care:“Other people [were steering] and it was hard not to be in control of decisions, and I’m the sort of person who resources sources” (P001). Two patient participant’s care was provided without them receiving direct consultation, with others having the decision-making role such as family. Family member P003-2 said, “Oh yeah, I have all the roles now”. One patient participant knew they did not have control: “I did not have a lot of decisions to make in my care”; and was not confident to communicate their treatment preferences. Three patient participants either wondered about negative reactions from staff or noticed staff members’ disapproval when the patient asserted their choices or made requests. Participant P001 said, “I remember some of them did mind [me deciding to stop weaning] because they were trying a couple of hours a day and then putting me back on regular [oxygen]”.
Patient participants were aware of treatments, surgeries, and diagnostic procedures they needed, and remembered explanations about these interventions. All patient participants were tracking their medications, and three identified when they were given too much medication. One participant said: “One day they over-medicated me for three days” (P002). Patient participants knew the effects of medications on their body, e.g., “they were very heavy on the brain” (P001); and wanted details of their medications. One patient participant noticed when nurses were not specific, such as a nurse saying, “It’s time for your medications. I’m giving you all your medications”; and wanted to ask, “like what are you giving me?” (P004). All four patient participants knew the steps in weaning off the ventilator and would check their respiratory monitors:
I was watching, as a matter of fact; I even had my wife turn the monitor so that I could see it at nighttime so if I happen to wake up and glance over to make sure what my oxygen levels were. And I didn’t want them to drop it below 90 or whatever the threshold was (P003).
Patient participants did not feel in control of the weaning process, and one patient stated weaning took place when they were asleep, without their knowledge. Patient participants wanted to know about all their medical interventions, not just medications: “I want to know the purpose for [the interventions] and these choices and to send people to talk to me” (P001). They wanted to ask their physician questions: “I was wondering how long I would have the catheter in because I was always getting a urinary tract infection” (P002).
Family participants said patient participants followed everything going on around them, even when they were not able to speak: “She controls, she’s tracking. She knows everything… I’m amazed” (P002-2). Patient participants heard information spoken at rounds, watched the monitors and staff.
Theme E: How Communication Occurs
Subthemes: Safety Issues from Lack of Communication, No Communication, Staff Do Not Understand, Unaided Communication, Partner Difficulty with Augmentative and Alternative Communication Systems.
All patient participants reported risks to their health and safety when they were not able to communicate with healthcare staff. Participant P004 reported not having a way to communicate that they were unable to breathe because of mucous blocking the airway: “When I didn’t have my mom and I needed a nurse and they couldn’t hear me, and I really had no way to communicate for help”. Patients couldn’t say they had received too much medication or that they needed careful transfers to avoid injury, so staff “just grabbed the top of my arm and my shoulder and yanked” (P003). One family participant referred to an error when transferring to another hospital: “There wasn’t a note in that system and if I wasn’t there with her, the nurse would have given her twice the blood thinner” (P004-2).
Every patient and family participant reported times when no communication was happening, saying “I get nothing a lot” (P001) and “some of them are not communicating at all” (P004-2). Patient participants understood that they could direct their care and report their symptoms if staff gave them a communication opportunity: “But just like taking the time to ask questions, and it might seem like a lot but it’s like OK do you want this, yes or no, yes or no” (P004). Patient participants needed communication opportunities and wanted ongoing explanations and updates: “They didn’t continue updating me and I think there were a lot of steps that needed to be taken” (P001). Family meetings did not happen as promised: “That never happened (a family meeting) they said it would, but I was never, if there was one I they never invited me” (P003-2).
Patients suggested staff did not use or understand how to implement patients’ alphabet chart or ICU Talk communication book (Etchels et al, 2013) or did not have the time (all the patients needed partner assisted scanning) and did not ask the right yes/no questions. A patient participant said, “They wouldn’t understand me most of the time, so it was very hard to explain, express my feelings, how I’m feeling at the time and what I needed” (P001).
Participants said they used unaided methods to communicate, including blinking or nodding/shaking their head to say yes and no, mouthing words with no voice, looking toward what they wanted, and gesturing toward people or objects in the room. Patients said that lip-reading was unreliable and skilled lip readers were often elsewhere, which meant patients had to wait to get their basic needs met. Family members acted as lip-readers for ICU staff who had difficulties and would act as the ‘translator’ during goals of care/end-of-life discussions .
Getting attention from healthcare staff was difficult for all patients when they used only unaided communication: “I would’ve liked to say, ‘come and see me’” (P002). Getting attention was particularly hard at night. As P003 said, “it’s scary waking up when you’re like you really need something but there is no-one there and just kinda hoping they’re gonna come in time”. The ICU in this study had no call bells, as there typically was a nurse at every bedside. Physical limitations meant three patient participants had no way of getting staff members’ attention in the usual ways and the fourth participant would hit the bed with his arm to get attention. That participant’s family member said: “They [nurses] would say “don’t do that” but he would want something” (P003-2).
Two patient participants encountered barriers to their use of high-tech communication: “A lot of nurses said, ‘I don’t know how to set that up’ and so that yeah that was a big obstacle” (P001). Patient participants wished people would be patient: “Everyone around me was ugh … the scanning is taking so long, but I want to articulate what I’d say, and this is the best way for me to” (P004). One patient participant found inadequate staff time meant not enough augmentative and alternative communication training for partners:
He did a great job trying to get, trying to teach me how to use it he did a very good job, and he was a really good communication person, but he really is you have to have the resource stuff it just wasn’t enough (P001).
There was a lack of space for accessing and using communication equipment: “[The] step-down [unit] was way too busy. Step down is like cramped. You can’t really put, and the nurses can’t deal with that, and they kept moving it” (P004-2).
Patient participants did not recommend using spelling only in goals-of-care/end-of-life meetings because it was slow and instead suggested a goals-of-care vocabulary for future ICU patients. They suggested patients could have one or two whole words or phrases that then could be expanded upon by ICU staff. Participants indicated that using a head mouse required too much fine motor control and was difficult for one patient-participant, and low-tech spelling-based systems were tiring for another .
It was tiring for me to do all this letters, especially you know if all I could do was shake my head, nod, or you know shake my head about the which if it is the right letter or not, and they would write down ok W-A-K-E you know (P003).
One patient participant suggested a goals of care vocabulary system should have whole words/phrases without having to spell everything.
Discussion
This study was conducted to learn more about how to support non-speaking ICU patients in goals-of-care and end-of-life conversations. Five themes emerged, some that echoed findings from studies of speaking patients, and others that were unique to AAC users.
Theme A: Communication partners
According to patient participants, communication partners did not always facilitate participation in healthcare discussions, meet patients’ basic needs, and wants, or give patients sufficient information and explanations about their health status and treatments. These findings suggest most goals-of-care/end-of-life discussions did not involve the patient and did not use a shared decision-making model (Elwyn et al., 2012; Bomhof-Roordink et al., 2019). This study corroborates work by Happ et al. (2007) where patients were informed after the discussion was completed rather than participating in the discussion. Family members’ suggestions of partner strategies (e.g., careful phrasing, positive and repeated information) are all suggestions designed to make information easier to understand and less emotionally loaded. This suggests that processing medical information was a complex task for them. Future patients may be aware of their family member’s difficulty processing healthcare information and consequently may need vocabulary to tell the healthcare team how to better communicate. This is consistent with the study by You et al.(2015) who identified family members’ difficulty understanding the limitations/complications of life-sustaining therapies, as one of the barriers to goals-of-care discussions.
All patient participants in this study approved of their family members’ role as a substitute decision maker but all patients reported a lack of updated information and involvement in goals of care/end of life from healthcare staff. Lindberg et al. (2015) found patient autonomy in six Swedish ICUs was an acknowledged dependence: patients wanted to have agency, co-partner in their care, be invited to participate in goals of care, and be recognised as a person. Patient participants said they were unaware of some decisions, and this is consistent with findings by You et al. (2014) who reported less than 30% concordance of use or non-use of life sustaining treatments with patients’ preferences, while in the ICU. Given that patients were able to recall details of their lack of inclusion in goals-of-care/end-of-life discussions, they likely were cognitively capable of participating at the time. Access to healthcare staff during interventions did not provide an adequate forum for goals discussions as all patient participants said they had unspoken opinions about their interventions, unasked questions, and did not get to direct their care plans. This finding suggests that even though there can be initial goals-of-care meetings with substitute decision-makers when patients are too ill to participate, additional meetings should be scheduled once patients are well enough to participate.
Theme B: Feelings and thoughts
Bomhoff-Roordink et al. (2019) did a systematic review of shared decision-making models and listening to patient’s concerns, preferences and values were elements noted in 65% of the models. The feelings and thoughts noted by participants in this study need to be conveyed using an AAC vocabulary system if future non-speaking ICU patients are given the opportunity to discuss their concerns. A previous study of mechanically ventilated patients in the ICU described patient experiences within themes having to endure and being out of control (Karlsson et al.,2011), similar to the findings in this study. Karlsson et al. (2011) described how patients with feelings of helplessness are more likely to submit to the will of other people. This tendency for submission could affect patients’ goals-of-care/end-of-life decisions. McCleod and Sherwin (2000) noted that oppression in medical decision making can occur based on the context patients find themselves in. It is unknown whether a shared decision-making context with space to hear from the non-speaking patient and family and avoidance of dominance by speaking participants may better support patient autonomy as this has not yet been studied. Participants in this study reported fear, isolation, feeling useless and a burden which are feelings described in other studies of intensive care patients (Khalaila et al., 2011; Tembo et al., 2015). The phrase “trapped in my body” used by one participant in this study is reminiscent of themes in the Tembo et al. (2015) study of patients who had mechanical ventilation in intensive care.
Theme C: Matters to talk about
Theme D: Control Power
Quotes from both family and patient participants showed that patients were watching and aware of their care but needed goals-of-care/end-of-life vocabulary to evaluate their care choices and question what they needed. Patients needed vocabulary to convey their thoughts as a decision maker, or to delegate that responsibility. Patients did not want to relinquish their own participation in goals-of-care/end-of-life discussions. Slatore et al. (2012) found that shared decisions with patients were usually based on care that was previously decided by physicians rather than decisions made by the patient. The findings in this study show patients did not participate in decision making as much as they would like, but it is uncertain what factors contributed to a lack of participation. They relied on a key worker, such as a nurse, social worker, or physician, who helped both participants and families with information and emotional support.
Comments by participants suggest there may have been a power imbalance between providers and patients, and a lack of patient agency. This power imbalance could be reduced if healthcare workers used techniques like those described by Kettunen et al. (2003), who identified two types of speech practices used by nurses that “facilitated the inclusion of patients’ perspectives and preferences and encouraged patients to express themselves” (p. 327). The first was use of “affective questions,” which gave patients choices of topics and asked their feelings and opinions. The second was using “tentative speech,” which, in an ICU context, might manifest as a phrase like, “This would be a good time to reposition you” vs. “I am going to reposition you now.” To use these techniques, staff need time and training, and augmentative and alternative communication users need vocabulary to direct healthcare workers to include them and direct the manner of that inclusion.
Theme E: How Communication occurs
AAC is feasible and effective in the intensive care unit with mechanically ventilated ICU patients, as identified by Zaga et al. (2019). Rodriguez et al. (2016) showed that with consistent access to tablets with speaking software, communication was less difficult for ICU patients. Szymkowicz et al. (2024) found that messages could be transmitted accurately with eye-tracking or a low-tech communication board. In the latter study, however, two-thirds of patients were not satisfied with the communication board, the most common AAC device in ICU (Zaga et al., 2019). Happ et al. (2014) found that even with SLP support, use of AAC was low (6%). These findings resonate with the patient participants’ suggestion that people need to understand what it is like not to communicate. It is not enough to provide a patient with alternative modalities and vocabulary: communication partner training is essential. The safety issues from lack of communication are reported in this study are similar to findings from Bartlett et al. (2008) who discovered multiple preventable adverse events for non-speaking participants due to drug errors (40%) or poor clinical management (32%).
Limitations
First, as this was a single-site study with narrow inclusion criteria, the sample size was small, making it unlikely everything was captured about non-speaking patients’ experience in the ICU. Findings such as safety concerns and lack of decision-making power, however, were similar to those of studies with larger samples (e.g., Bartlett et al., 2008) suggesting that the themes have broader application. Second, this study was limited to communication needs for goals-of-care and end-of-life discussions, although key themes could apply to other patient communication interactions. Third, there was a risk of recall bias by patient participants, who may have been medicated and sleepy in the ICU and their experience was up to a year prior to the interview. Comments from family members were similar, however, which supports the trustworthiness of patients’ comments. Fourth, it is recognized that FC has a potential bias from working in the ICU, which could have predisposed FC to negative themes. It was important to have an augmentative and alternative communication specialist complete the interviews, to probe participants’ experiences using augmentative and alternative communication modalities, and potential bias was mitigated by involving researchers with no ICU experience (LT) or no professional training (TC) in analysis.
Conclusion
Results of this study represent the perspectives of a group of adults who had been temporarily non-speaking in the ICU from their medical condition, and their chosen family members, each of whom reflected on their goals-of-care/end-of-life and treatment consent discussions. Participants’ comments provide valuable insights into the experiences while an ICU patient who is temporarily unable to speak. The findings show that patients who are non-speaking have many unmet communication needs related to goals of care/end of life. There is compelling evidence that patients need an augmentative and alternative communication vocabulary system that is specific to goals-of-care/end-of-life discussions in the ICU. Developing this tool would enable patients to have discussions, get information and care from ICU healthcare staff. With such a tool they could discuss their feelings and thoughts, talk about ICU-specific topics, and negotiate control and power in a way that meets the needs of medical, physical, and interpersonal contexts in which communication happens. It is acknowledged that the solution to greater patient participation in goals-of-care discussions is likely to be multifactorial. Factors such as the level of training of communication partners and support to remove to barriers to use of AAC in the ICU will also be important.
Acknowledgements
The authors wish to thank the participants for sharing their time and experiences, and Kelly Ann Moschopoulos who helped with the consent process.
Funding and conflict of interest: There was no funding provided for this work and there are no known conflicts of interest.