(002).png)
Cultural adaptation in Quebec of the COMHON index: a tool for assessing the risk of pressure injury in critically ill patients
Annie Perron, MSc, RN, Gwenaelle De Clifford-Faugere, PhD, RN, Cylia Parent-Faubert, BSc, RN, Miriam Predan-Lépine, NP, Angel Cobos-Vargas, RN, Manuel Colmenero, MD, PhD, an d Anaïs Lacasse, PhD
Background: Pressure injuries (PIs) are preventable and particularly frequent complications that arise in intensive care units (ICUs). To date, no French-language PI risk assessment tool has been specifically developed for ICUs. The COMHON Index is used to assess the risk of developing PI specifically among patients admitted to ICUs. It is available in several languages, including English, Japanese and Spanish, and has demonstrated promising psychometric properties.
Purpose: The goal of this study was to perform the French translation and cultural adaptation of the COMHON Index for the Quebec (Qc) critical care environment, resulting in the COMHON-Qc Index.
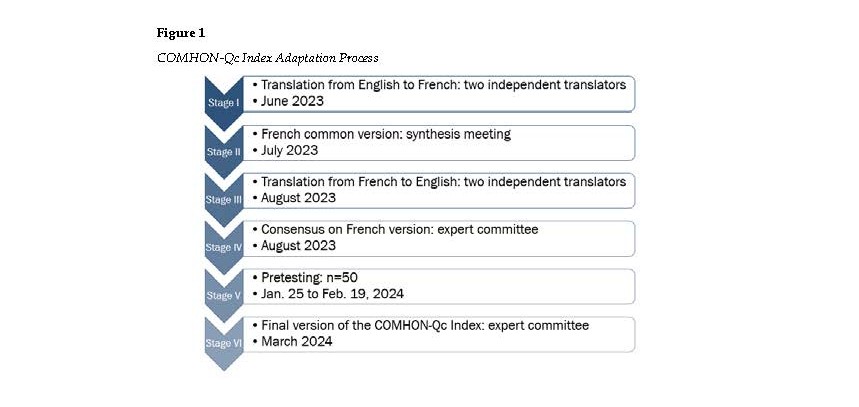
Method: The Quebec version of the tool was developed as per the guidelines for the process of cross-cultural adaptation established by Beaton et al. (2000): I) two forward translations into French; II) synthesis; III) two back translations; IV) expert committee review; V) pretesting; and VI) final version.
Results: Stages I through IV were performed by a committee made up of 5 experts. During stage V, 51 ICU nurses participated in a pretest to assess the clarity of the COMHON-Qc Index, which enabled the development of a final version by a committee of experts during stage VI.
Discussion and conclusion: The items in the COMHON-Qc Index are comprehensible and relevant for the nursing practice in Quebec. Future assessment of the tool’s psychometric properties is now required to support its implementation.
Implications for Nurses
PIs are a preventable complication. Their detection enables the implementation of preventative measures.
Nurses play a key role in PI risk assessment and prevention. An appropriate tool can support nurses in effectively fulfill this role in ICUs.
The COMHON-Qc Index is developed specifically for ICUs. To our knowledge, this is the first such index in French developed to meet ICU-specific needs.
Background and Purpose
Pressure injuries (PIs) are a significant concern in healthcare facilities. They lead to longer hospital stays and pose a substantial financial burden, with costs reaching up to $CA 90,000 for hospital-acquired stage 4 PI (Norton et al., 2025; Vanderwee et al., 2011). Furthermore, in 70% of cases, PIs are avoidable complications (Norton et al., 2025). In fact, simple interventions such as proper skin care and frequent repositioning reduce the risk of PI (European Pressure Ulcer Advisory Panel et al., 2019).
According to studies and data from healthcare facilities, the prevalence of PIs among hospitalized patients varies between 0.4 and 36.8% (Houghton, 2021; Li et al., 2020). The highest number of PI cases are observed in ICUs (prevalence between 7.78 and 46.7%) due to the critical condition of the patients (Rubulotta et al., 2022; VanGilder et al., 2021). In Canada, the prevalence of PI in ICUs ranges from 14% to 42% (Leblanc et al., 2019). Factors at play in the high prevalence of PIs in such units include patient hemodynamic profiles and levels of consciousness, along with the use of medical devices specific to critical care settings (e.g., BiPAP masks, endotracheal tubes, or pulse oximeter sensors) (Ítalo Lennon Sales de et al., 2020). Through detection of at-risk patients, the number of PIs could significantly reduce through the implementation of preventative measures (Cobos-Vargas et al., 2023; Labeau et al., 2021; Lovegrove et al., 2020). Considering the impact of PI on patients, and given their preventable nature and economic impact, it is critical to effectively detect at-risk ICU patients using a tool designed specifically for critical care settings (Labeau et al., 2021).
Several clinical tools are available to detect patients at risk of PIs, including the Braden Scale (Braden & Bergstrom, 1989), which is available in French and commonly used in Quebec hospitals (Norton et al., 2025). However, these tools were not specifically designed for ICU patients (Lima-Serrano et al., 2018), and the related particularities that impact the risk of PI, such as the level of consciousness, hemodynamic profile and the use of vasopressor agents and mechanical ventilation (Cox, 2017; Fulbrook & Anderson, 2015). The risk factors for developing a PI vary across clinical environments, and the specificity and sensitivity of the same risk assessment tool vary depending on the clinical setting in which it is used (Moore & Patton, 2019). Additionally, the literature shows a lack of consensus on assessment frequency and the threshold an ICU patient would be considered at risk according to the Braden Scale (Lima-Serrano et al., 2018). When risk assessments are conducted on the day of ICU admission, the Braden Scale demonstrates low sensitivity and positive predictive value of 0.3% and 8.1%, respectively (Lima-Serrano et al., 2018).
The COMHON (level COnsciousness, Mobility, Hemodynamics, Oxygenation, Nutrition) Index, originally in Spanish, was created to assess the risk of developing PI specifically among patients admitted to ICUs (Cobos Vargas, 2013). Cross-cultural adaptations of the COMHON Index were performed in English, Japanese and Mandarin (Lovegrove et al., 2022). Many studies have validated the English version of the tool (Fulbrook & Anderson, 2015; Ítalo Lennon Sales de et al., 2020; Lovegrove et al., 2020). The English version of the COMHON Index was compared to three other PI risk assessment tools: the Braden Scale, the Norton Scale and the Waterlow Scale (Fulbrook & Anderson, 2015). In this study, the COMHON Index received the highest precision score in terms of PI risk assessment (Cohen’s kappa for the COMHON Index: 0.90; for the Braden Scale: 0.66; for the Waterlow Scale: 0.47) (Fulbrook & Anderson, 2015). It also proved most sensitive to slight changes in medical conditions, thus making it more effective in detecting at-risk individuals (Fulbrook & Anderson, 2015). Moreover, the COMHON Index showed a strong negative correlation (-0.7) with the Braden Scale (negative due to the Braden Scale’s inverted score, p <0.001) (Fulbrook & Anderson, 2015). However, no French version of the COMHON Index currently exists and has not been validated in a Quebec setting, Quebec being the only Canadian province where French is the only official language (84% of the Quebec population is French-speaking) (Canadian Heritage, 2024).
Several authors have emphasized the importance of the cross-cultural adaptation process to ensure that clinical tools are both valid and reliable within the population where they are used, considering the local language and cultural context (Beaton et al., 2000; Lauzier et al., 2023; Sousa & Rojjanasrirat, 2011). In Quebec, researchers in health sciences have undertaken numerous projects aimed at adapting assessment tools across various clinical fields (Beauchamp et al., 2021; Beaumier et al., 2019; Lacasse et al., 2017; Lavoie et al., 2021; Perron et al., 2022).
The aim of this study was to perform a cross-cultural adaptation the COMHON Index to French and to provide a culturally adapted tool for clinicians in Quebec ICUs.
Method
Tool description
The COMHON Index contains five items: level of consciousness, mobility, hemodynamics, oxygenation, and nutrition. The first section simply presents the items, while the second provides a detailed explanation of each component along with its definition. The items are assessed according to the severity of the individual’s medical condition scored on a scale from 1 to 4. The final score, obtained by adding the result of each item, indicates one of three levels of risk of developing PI: 5 to 9 (low risk), 10 to 13 (moderate risk) and 14 to 20 (high risk) (Lovegrove et al., 2020).
Cross-cultural adaptation of the COMHON Index
The Quebec version of the COMHON Index was developed as per the guidelines for the process of cross-cultural adaptation of questionnaires established by Beaton and his collaborators (2000). For practical reasons, we used the English version of the tool as a source document. Permission from the original authors of the original version (Spanish and English) was obtained beforehand. Figure 1 maps out the adaptation process followed.
Stage I: Two forward translations
Two French translations were performed independently by two bilingual nurses whose native language was French and who had never used the COMHON Index in their practice. One of the nurses was from Quebec and the other was from France and had lived in Quebec for several years. One of the translators worked in the field of critical healthcare while the other has expertise in cross-cultural adaptation of measurement instruments. Each translator delivered a detailed written report capturing their suggestions and comments pertaining to the translation and any concerns/issues related to specific sentences.
Stage II: Synthesis
As recommended by the guidelines for cross-cultural adaptation (Beaton et al., 2000), an expert committee, composed of the aforementioned translators and a facilitator with expertise in critical care, sat down to synthesize the translations and discuss the reports produced in stage I. This led to the development of one common version of the COMHON-Qc Index, a Quebec adaptation in French of the original COMHON Index.
Stage III: Two back translations
Using the version of the COMHON-Qc developed in stage II as a source document, two independent translators, whose native language was English and who lived in Quebec, performed two back translations (one each) into English. One of the translators was a nurse with experience in critical healthcare; the other was not from the field of healthcare. Neither translator had any prior knowledge of the original English version of the COMHON Index as recommended by guidelines for cross-cultural adaptation (Beaton et al., 2000). Following stage III, a detailed report including the original English version, the Quebec adaptation (stage II), and both English back translations (stage III) was produced.
Stage IV: Expert committee
An expert committee came together to reach a consensus on the prefinal version of the COMHON-Qc Index. As recommended by Beaton and his collaborators (2000), the committee composed both translators from stage I (both native French speakers; one specialized in the field of intensive care), the translator with experience in nursing from stage III, and a facilitator with expertise in critical care. These experts had previously received the comprehensive report from stage III. First, the committee reviewed the overall results of the two forward translations from stage I and the two back translations from stage III and reached a consensus on the semantic choices and accuracy for the prefinal version of the COMHON-Qc Index in terms of the concepts covered. Next, the committee performed contextual adaptations between the original English version and the Quebec version to better reflect the practice setting of French-speaking nurses in Quebec, the outcome of which was the prefinal version of the COMHON-Qc Index.
Stage V: Pretesting
The Beaton guidelines (Beaton et al., 2000) for the cross-cultural adaptation of self-report measurement tools recommend pretesting the prefinal version among 30 to 40 individuals from the target setting. Once ethical approval was obtained (Ethics Certificate No. 2023-10_Perron A), the prefinal version of the COMHON-Qc Index was pretested among a sample of nurses from the province of Quebec using convenience and snowball sampling. The participant selection criteria were as follows: 1) nurse and member of the Ordre des infirmières et infirmiers du Québec (OIIQ); 2) at least 6 months of recent experience (past 5 years) in an ICU; 3) ability to understand and complete a questionnaire in French. An invitation was sent to the professional contacts of the members of the research team by email and through social media. Also, an invitation was shared by the Regroupement des infirmières et infirmiers en soins intensifs du Québec (RIISIQ) and the Réseau de recherche en interventions en sciences infirmières du Québec (RRISIQ). Participants completed the web questionnaire anonymously through Microsoft® Forms. The first page of the form outlined the project with sufficient information to allow for free and informed consent. The act of completing the questionnaire constituted in and of itself agreement by the participants. Participants were asked to indicate if each item was clearly formulated and to add comments, if needed, for both sections: 1) items from the COMHON Index; and 2) items with definitions, as per the layout of the original COMHON Index.
Stage VI: Final version
The expert committee examined the pretesting results from stage II. The comments submitted by the participating nursing staff were considered to further clarify the French version of the COMHON Index. The final version, following adaptations, is presented in the results section. Such a version was discussed with the authors of the original COMHON Index.
Results
During stage V, 50 individuals took part in the pretesting process of the prefinal version of the COMHON-Qc Index. A sample of 30 to 40 individuals was required (Beaton et al., 2000), however, a higher number of nurses completed the web questionnaire in a very short period of time. Table 1 shows an overview of the pretesting results along with the adjustments made during stage VI.
The participants made 33 comments on the section of the COMHON-Qc Index, putting forth the items without the definitions; they made 67 comments on the section, including the items and the definitions. One of the main adaptations of the COMHON Index to the Quebec setting was a formatting change aimed at simplifying presentation and adding item definitions alongside the scales. This formatting saves users the burden of having to go back and forth between where the scores were to be entered and the definitions needed to complete the scores. In fact, between 32 and 41 participants reported that the items without definitions were completely intelligible, while this number increases from 38 to 49 for the complete version with definitions. Furthermore, by adding the definitions to the items, 17 of the 33 comments regarding the section outlining the items without definitions were addressed.
Several comments regarding the overall questionnaire (n = 18/110) suggested splitting certain categories or further specifying health conditions. However, the research team decided not to implement these changes, as subdividing these items would have no meaningful impact on PI risk assessment. For example, one participant stated that there is a difference between a Richmond Agitation Sedation Scale (RASS) score of -3, -4, and -5, and that the RASS/Glasgow Coma Scale (GCS) scores must be accurate during the evaluation. Clinically speaking, there is a difference. However, the COMHON Index groups the assessment of level of consciousness into four levels (i.e. Awake and alert (RASS 0, + 1) (Glasgow 15), Agitated, restless, confused (RASS > 1) (Glasgow 13 – 14), Sedated but responsive (RASS -1 to -3) (Glasgow 9 – 12) and Coma, sedated and unresponsive (RASS < -3) (Glasgow < 9)), as the risk of pressure injury does not necessarily increase with each variation in the state of consciousness according to RASS and Glasgow (Fulbrook & Anderson, 2015). We therefore added an explanatory note before the questionnaire items to address such comments and concerns among healthcare professionals during clinical assessment.
The expert committee explored the clinical use of the COMHON-Qc Index and considered the need to review its layout to facilitate daily assessments by healthcare professionals. Moreover, the preventive interventions required according to COMHON scale risk level, which has been develop by a group of international experts were added to the back of the tool to guide healthcare professionals in preventing PIs by promptly taking appropriate measures (Lovegrove et al., 2020).
Likewise, the expert committee examined the best approach to clarify nutrition-related items in response to comments made by nurses about the notion of “needs met” by the patient. As underlined by three nurses, a person can have a normal diet without their nutritional needs being met. A meeting was held with the authors of the original COMHON Index. Such authors mentioned that the nutrition-based items had actually sparked the most discussion during previous work on the tool. Following these exchanges, the comments on the clarity of such items, and the guidelines on the effects of nutritional status on PIs (Munoz & Posthauer, 2022; National Pressure Injury Advisory Panel et al., 2025), the expert committee decided to add the notion of “met nutritional needs” to the second point of Nutrition. The final version of the tool is shown in Table 2.
Discussion
The goal of this study is to perform a cross-cultural adaptation of the COMHON Index to the cultural setting of Quebec ICUs. The process enabled the creation of a French-language PI risk detection tool considered comprehensible by nurses working in such units. The addition of recommended interventions based on risk makes this tool both practical and comprehensive in supporting clinical decision-making among such healthcare professionals.
The use of a questionnaire by individuals of different origins than those of the tool’s target population requires both translation and cultural adaptation to preserve content validity for the target population (Beaton et al., 2000). In this project, all stages were completed in strict accordance with the cross-cultural adaptation process described by Beaton et al. (2000) in Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. The cultural adaptation setting and certain modifications warrant further discussion.
During stage III (two back translations), the back translations into English showed some inconsistencies with the original version used in stage 1 (two forward translations). For instance, the native English-speaking expert from Quebec preferred formulations such as “Very limited but tolerates changing positions” rather than “Very limited but tolerates position change,” and used “respiration” instead of “breathing.” These minor discrepancies likely reflect regional variations in English usage. While the original English version of the tool was adapted by an Australian team, our translation involved a Quebec-based expert, which may explain subtle lexical and syntactic differences.
During pretesting (stage V), the Braden Scale was mentioned three times by participants, suggesting to use the same items as that scale for the COMHON-Qc Index. Notably, the Braden Scale is widely used in Canadian hospitals (Registered Nurses’ Association of Ontario (RNAO), 2024). It is therefore possible that participants compared the two tools and suggested aligning the items for easier use. However, the Braden Scale differs in that it requires a projection over time, while the COMHON-Qc Index reflects the health status upon assessment and must be repeated every shift. The notion of time in the Braden Scale limits its use in ICU settings, and this tool was not developed with consideration of the specific risk factors associated with ICU (Fulbrook & Anderson, 2015). This is not the case for the COMHOM-Qc Index. In ICUs, patients’ medical condition can deteriorate rapidly (Lavoie et al., 2014), potentially causing substantial changes to the risk of PI at any given time (Cox, 2017; Rubulotta et al., 2022). These realities underscore the importance of using a tool designed specifically for ICUs to assess the risk of PI among such patients. That said, management teams must ensure the proper training of nurses before the implementation of the COMHON-Qc Index in ICUs, especially if the Braden Scale is already in use. The implementation strategies for Best Practice Guidelines proposed by the RNAO (2024) can be useful to support a successful implementation.
Regarding the interpretation of the COMHON Index results, a Delphi study by Lovegrove et al. (2020) identified an association between the level of risk based on the COMHON Index and clinical preventive interventions. Their study, involving 67 international experts, provides direct guidance for clinical practice (Lovegrove et al., 2020). Given the impact of preventive interventions on PIs, our expert committee decided to add the interventions recommended by Lovegrove et al. (2020) to those found in the tool. Such interventions address, for instance, the frequency of position changes and the need for pressure relief. They also recommend assessing the PI risk using the COMHON Index every eight hours (Lovegrove et al., 2020). However, the literature offers no consensus on the frequency of PI risk assessments (Lima-Serrano et al., 2018), and further research on optimal assessment frequency is needed. Adding these interventions will guide clinical practice and, ultimately, decrease the risk of PI in Quebec ICUs.
The main adaptation made to the tool is related to the Nutrition item. This item generated the highest number of comments during pretesting. The authors of the original tool in Spanish also highlighted that this item sparked the most discussion during previous projects. It is also noteworthy that no pretesting of the COMHON Index was performed to assess clarity during the English adaptation. Based on the comments and suggestions of the participating nurses concerning the importance of meeting the nutritional needs of patients to prevent PIs and according to the latest guidelines (Munoz & Posthauer, 2022; National Pressure Injury Advisory Panel et al., 2025), the committee decided to add “dans le but de combler ses besoins” to point 2 of the Nutrition item. This addition ensures the creation of a comprehensible tool adapted to the cultural setting of Quebec, and in line with recent empirical data.
Limitations and future studies
While the present study follows the guidelines for the cross-cultural adaptation of measurement tools (Beaton et al., 2000), some limitations should be acknowledged. As the sociodemographic data of participants was not collected it was not possible to verify the sample’s diversity to ensure an optimal representation of nurses in Quebec. Furthermore, all participants who took part in pretesting were from the province of Quebec. Quebec does hold Canada’s largest population of French speakers; however, the research team recognizes the existence of several French-speaking communities outside of Quebec and that these communities were not included by this study. Cross-cultural adaptation represents the initial phase in the adaptation and validation process (Beaton et al., 2000). Studies on the psychometric properties of the COMHON-Qc Index are now required (Mokkink et al., 2010).
Conclusion
The present study led to the French adaptation of a PI risk assessment tool designed specifically for ICUs. Improving care quality and reducing PI risks for hospitalized patients can be accomplished through accurate assessment of PI risks and implementing appropriate preventive interventions. The COMHON-Qc Index is therefore a valuable and relevant resource for nursing staff in Quebec ICUs. The present publication of the COMHON-Qc Index is the first step towards implementation by various teams in clinical settings and its assessment in terms of clarity, validity and sensitivity to change.
Funding and conflict of interest
The authors declare no funding and no conflict of interest